Vertebral Metastasis¶
Summary

- Vertebral metastases are secondary malignant lesions in the spine from distant primary tumours
- Common primaries include breast, lung, prostate, thyroid, and renal cell carcinomas
Pathophysiology¶
- Metastatic spread to vertebrae occurs via:
- Haematogenous dissemination
- Direct extension from paravertebral masses
- Lymphatic spread (less common)
- Tumour cells colonise bone marrow and induce osteoclastic or osteoblastic activity
- Lesions can be:
- Osteolytic (bone destruction)
- Osteoblastic (new bone formation)
- Mixed
Demographics¶
- Most common in adults aged 40-65 years
- Slightly more prevalent in males
- Incidence increases with age
- Accounts for approximately 70% of all osseous metastases
- Thoracic spine most commonly affected (60-70%), followed by lumbar (20%) and cervical (10%) regions
Diagnosis¶
- Clinical presentation:
- Back pain (often worse at night or when recumbent)
- Neurological deficits (radiculopathy, myelopathy)
- Pathological fractures
- Spinal cord compression (in advanced cases)
- Laboratory tests:
- Elevated tumour markers (e.g., PSA, CA 15-3)
- Increased alkaline phosphatase
- Hypercalcaemia
- Biopsy:
- CT-guided or open biopsy for definitive diagnosis and primary tumour identification
Imaging¶
- Plain radiographs:
- Limited sensitivity (50-70%)
- May show lytic or blastic lesions, vertebral collapse, or pedicle erosion
- CT:
- Higher sensitivity than radiographs
- Better visualisation of bone destruction and cortical integrity
- Useful for assessing stability and fracture risk
- MRI:
- Gold standard for detecting vertebral metastases
- T1-weighted images: hypointense lesions
- T2-weighted images: hyperintense lesions
- Contrast-enhanced sequences improve lesion detection
- Whole-body MRI useful for staging
- Bone scintigraphy:
- High sensitivity but low specificity
- Useful for whole-body screening
- PET/CT:
- High sensitivity and specificity
- Allows for detection of both osseous and extra-osseous metastases
- 60-year-old patient with breast cancer presented with acute back pain.
- CT showed a compression fracture of L3, a lucent region, and bulging of the posterior cortex into the vertebral canal.
- MRI showed abnormal signal in the whole vertebral body.

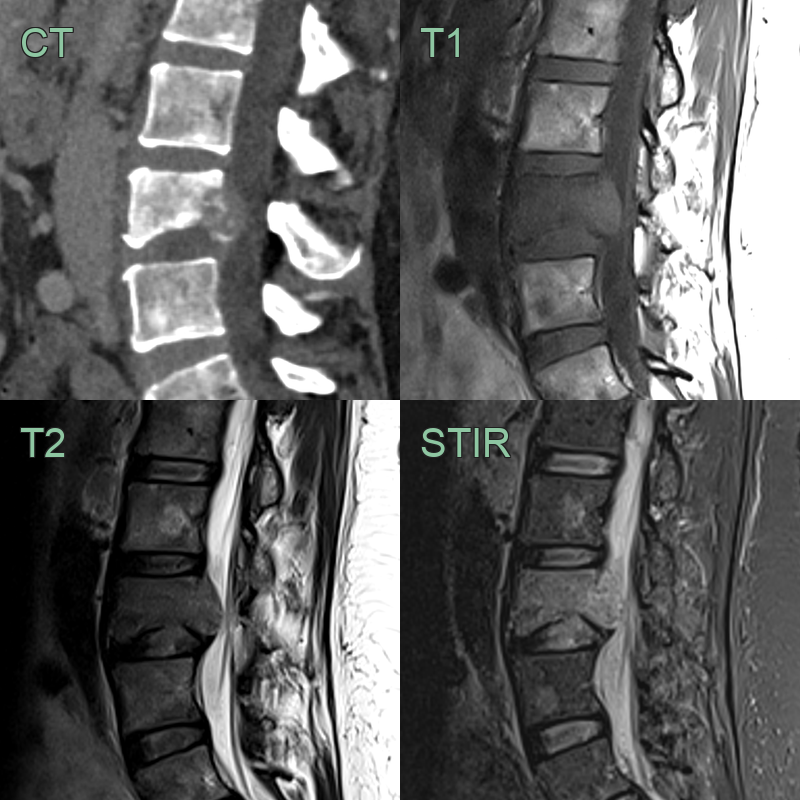
- 60-year-old patient with lung cancer presented with back pain.
- MRI shows lesions in the T12 (causing a compression fracture) and L2 vertebral bodies that were STIR hyperintense and T2 and T1 hypointense.
Treatment¶
- Multidisciplinary approach involving oncology, radiology, and orthopaedics
- Pain management:
- Analgesics (NSAIDs, opioids)
- Bisphosphonates or denosumab for bone pain
- Radiotherapy:
- External beam radiation for localised pain relief
- Stereotactic body radiotherapy for oligometastatic disease
- Surgery:
- Spinal stabilisation for impending or actual pathological fractures
- Decompression for spinal cord compression
- Minimally invasive procedures:
- Vertebroplasty or kyphoplasty for painful osteolytic lesions
- Radiofrequency ablation for small, localised lesions
- Systemic therapy:
- Chemotherapy, hormonal therapy, or targeted therapies based on primary tumour type
- Immunotherapy:
- Emerging option for certain tumour types (e.g., melanoma, renal cell carcinoma)
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Osteoporotic fracture | Lack of focal lesion, diffuse osteopenia |
| Degenerative disc disease | Preserved vertebral body height, disc space narrowing |
| Osteomyelitis | Contiguous disc space and end-plate involvement; paraspinal soft tissue; T1 hypointense and STIR hyperintense crossing disc |
| Multiple myeloma | Diffuse osteopenia; punched-out lytic lesions; T1 hypointense and STIR hyperintense; may show diffuse marrow involvement |
| Primary bone tumour | Typically single lesion; posterior element involvement common; chondroid or osteoid matrix on CT |
| Paget's disease | Increased bone density with bone enlargement and cortical thickening; "picture frame" or "ivory vertebra" appearance |
| Tuberculosis of spine | Disc space involvement with end-plate erosion; gibbus deformity; paraspinal and psoas abscess with rim enhancement |
| Hemangioma | Characteristic "polka-dot" appearance on CT; high T1 and T2 signal; no destructive bone changes |
| Lymphoma | Preservation of disc space with permeative infiltration; soft tissue mass; homogeneous on MRI |
| Aneurysmal bone cyst | Expansile lytic lesion with multiple fluid-fluid levels on MRI; thin cortical shell |