Vestibular Schwannoma¶
Summary

- Benign tumour arising from Schwann cells of the vestibular nerve
- Typically presents with unilateral hearing loss, tinnitus, and balance disturbances
- Characteristic imaging finding: enhancing mass in the cerebellopontine angle cistern
Pathophysiology¶
- Originates from Schwann cells of the vestibular portion of CN VIII
- Slow-growing, encapsulated tumour
- May compress adjacent structures, including:
- Cochlear nerve
- Facial nerve
- Brainstem
- Cerebellum
- Associated with NF2 gene mutations in some cases
Demographics¶
- Incidence: 1-2 per 100,000 person-years
- Peak age: 40-60 years
- Slight female predominance
- Bilateral tumours associated with Neurofibromatosis Type 2 (NF2)
Diagnosis¶
- Clinical presentation:
- Gradual, unilateral sensorineural hearing loss (95%)
- Tinnitus (63%)
- Balance disturbances (61%)
- Facial numbness or weakness (17%)
- Audiometry:
- Asymmetric sensorineural hearing loss
- Poor speech discrimination
- Vestibular function tests:
- Caloric testing may show reduced vestibular function
Imaging¶
- MRI (gold standard):
- T1-weighted: isointense to hypointense
- T2-weighted: heterogeneous signal intensity
- Contrast-enhanced T1: intense, homogeneous enhancement
- Characteristic "ice cream cone" appearance in internal auditory canal
- CT:
- Widening of internal auditory canal
- Erosion of petrous bone in larger tumours
- Cystic changes and heterogeneous enhancement more common in larger tumours
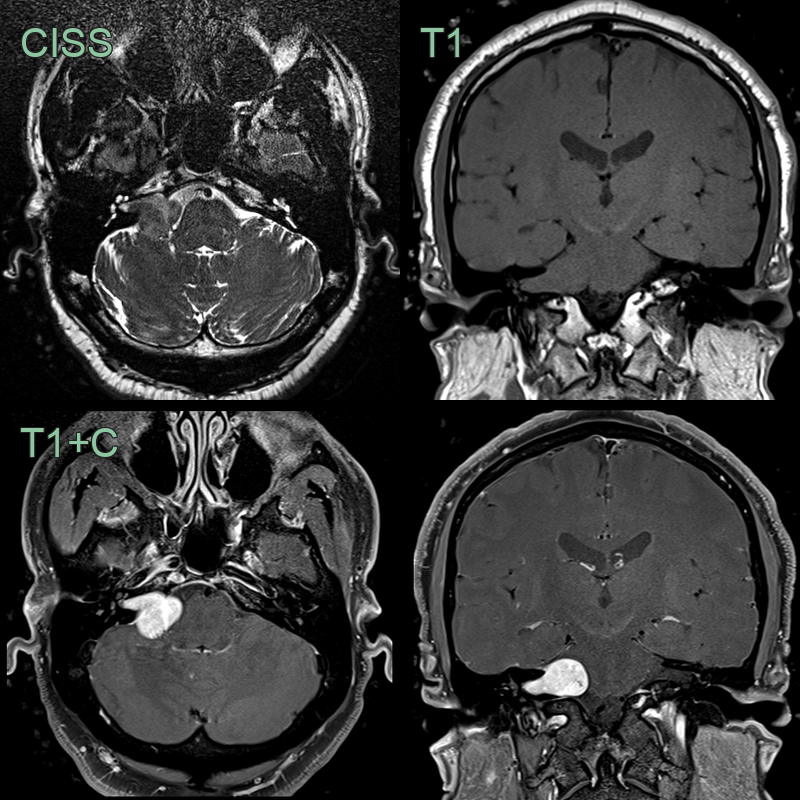
- 40-year-old presenting with right sided sensorineural hearing loss.
- MRI showed an avidly enhancing lesion filling the right internal auditory canal and cerebellopontine angle cistern.
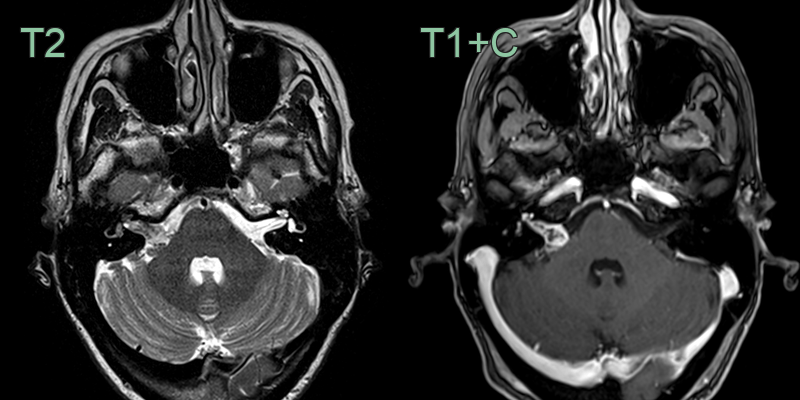
- 50-year-old patient present with total right-sided sensorineural hearing loss.
- MRI showed an enhancing lesion in the internal auditory canal.
- Enhancement and loss of fluid signal within the cochlea and vestibule indicated labyrinthine extension of the schwannoma.
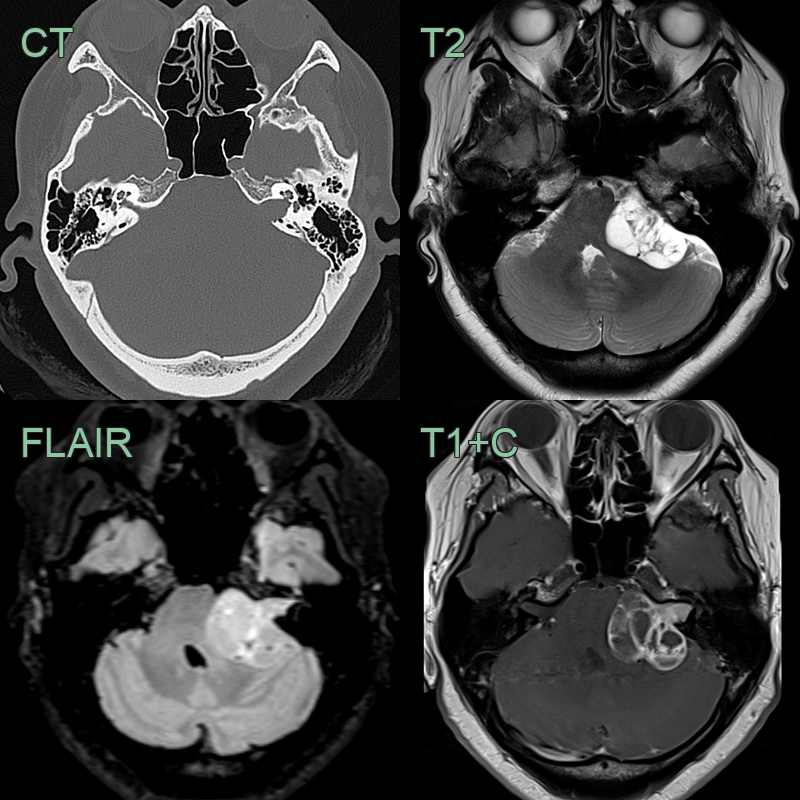
- 30-year-old patient with left sided facial weakness and sensorineural hearing loss.
- CT showed a widened internal auditory canal due to a large solid-cystic lesion centred on the left cerebellopontine angle cistern.
Treatment¶
- Observation with serial imaging for small, asymptomatic tumours
- Microsurgical resection:
- Retrosigmoid, translabyrinthine, or middle fossa approach
- Goal: complete tumour removal with preservation of facial nerve function
- Stereotactic radiosurgery:
- Option for smaller tumours (<3 cm)
- Aims to arrest tumour growth rather than remove the tumour
- Hearing preservation strategies:
- Cochlear implantation
- Auditory brainstem implantation
- Management decisions based on:
- Tumour size and growth rate
- Patient age and comorbidities
- Hearing status
- Patient preferences
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Meningioma | Typically has a dural tail on MRI; often enhances more homogeneously |
| Facial nerve schwannoma | Involves the facial nerve canal; may cause facial weakness |
| Cholesteatoma | Appears hypointense on T1-weighted MRI; does not enhance with contrast |
| Arachnoid cyst | Non-enhancing, CSF-like signal on all MRI sequences |
| Metastasis | Often multiple CPA lesions; irregular margins; may show adjacent bone destruction |
| Glomus jugulare tumour | "Salt and pepper" appearance on T2-weighted MRI; extends into jugular foramen |
| Epidermoid cyst | Restricted diffusion on DWI; irregular margins |
| Aneurysm | Flow voids on MRI; enhances on CTA or MRA |
| Multiple sclerosis plaque | Ovoid lesions; often multiple; may enhance with contrast in active phase |
| Lipoma | Hyperintense on T1-weighted images; suppresses on fat-saturated sequences |