Varicella Zoster Virus (VZV) Vasculitis¶
Summary
- VZV vasculitis is a rare but serious complication of VZV infection, affecting cerebral arteries
- Characterised by stroke-like symptoms and arterial wall inflammation on imaging
- Diagnosis relies on clinical presentation, VZV PCR, and neuroimaging findings
Pathophysiology¶
- VZV reactivation in cranial nerve or dorsal root ganglia leads to:
- Direct viral invasion of arterial walls
- Inflammatory response causing vessel wall thickening and stenosis
- Affects both large and small cerebral vessels:
- Large-vessel vasculopathy: mainly in immunocompetent adults
- Small-vessel vasculopathy: predominantly in immunocompromised patients
Demographics¶
- Incidence: rare, exact prevalence unknown
- Risk factors:
- Advanced age (>60 years)
- Immunosuppression (HIV, organ transplantation, chemotherapy)
- Can occur in both children and adults
- More common in individuals with a history of herpes zoster
Diagnosis¶
- Clinical presentation:
- Acute onset of focal neurological deficits
- Headache, altered mental status
- May be preceded by herpes zoster rash (not always present)
- Laboratory findings:
- VZV DNA detection in cerebrospinal fluid (CSF) by PCR
- Anti-VZV IgG antibodies in CSF
- Differential diagnosis:
- Other causes of stroke
- Central nervous system infections
- Autoimmune vasculitis
Imaging¶
- Magnetic Resonance Imaging (MRI):
- Acute ischaemic lesions in various vascular territories
- T2/FLAIR hyperintensities in affected areas
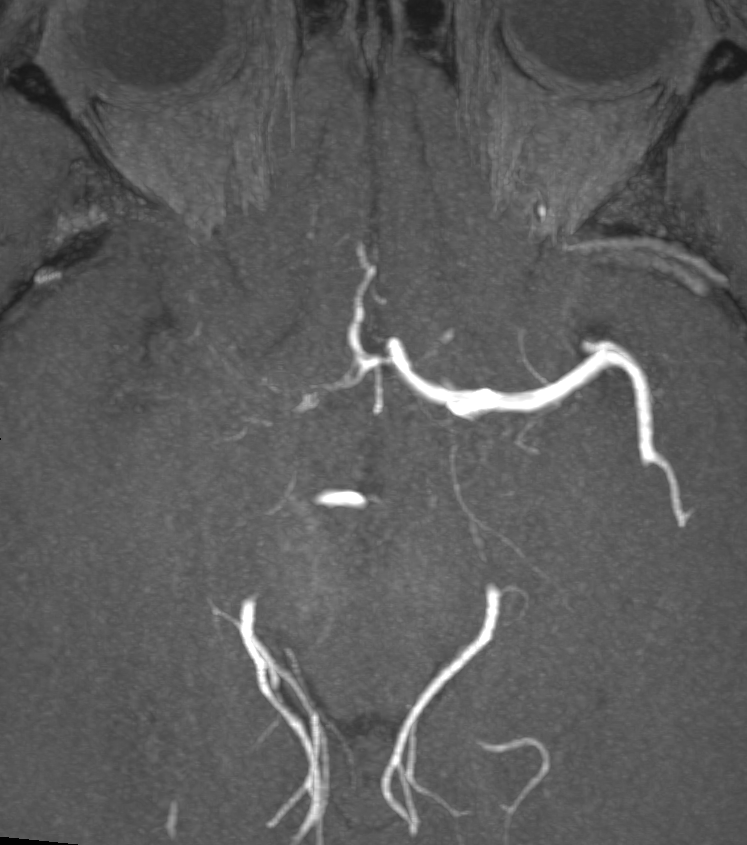
- Magnetic Resonance Angiography (MRA):
- Focal or multifocal stenosis of cerebral arteries
- Beading appearance of affected vessels
- Computed Tomography Angiography (CTA):
- May show similar findings to MRA
- Vessel wall imaging:
- Contrast enhancement of affected arterial walls
- Digital Subtraction Angiography (DSA):
- Gold standard for detailed vascular assessment
- Demonstrates stenosis, occlusion, or beading of affected arteries
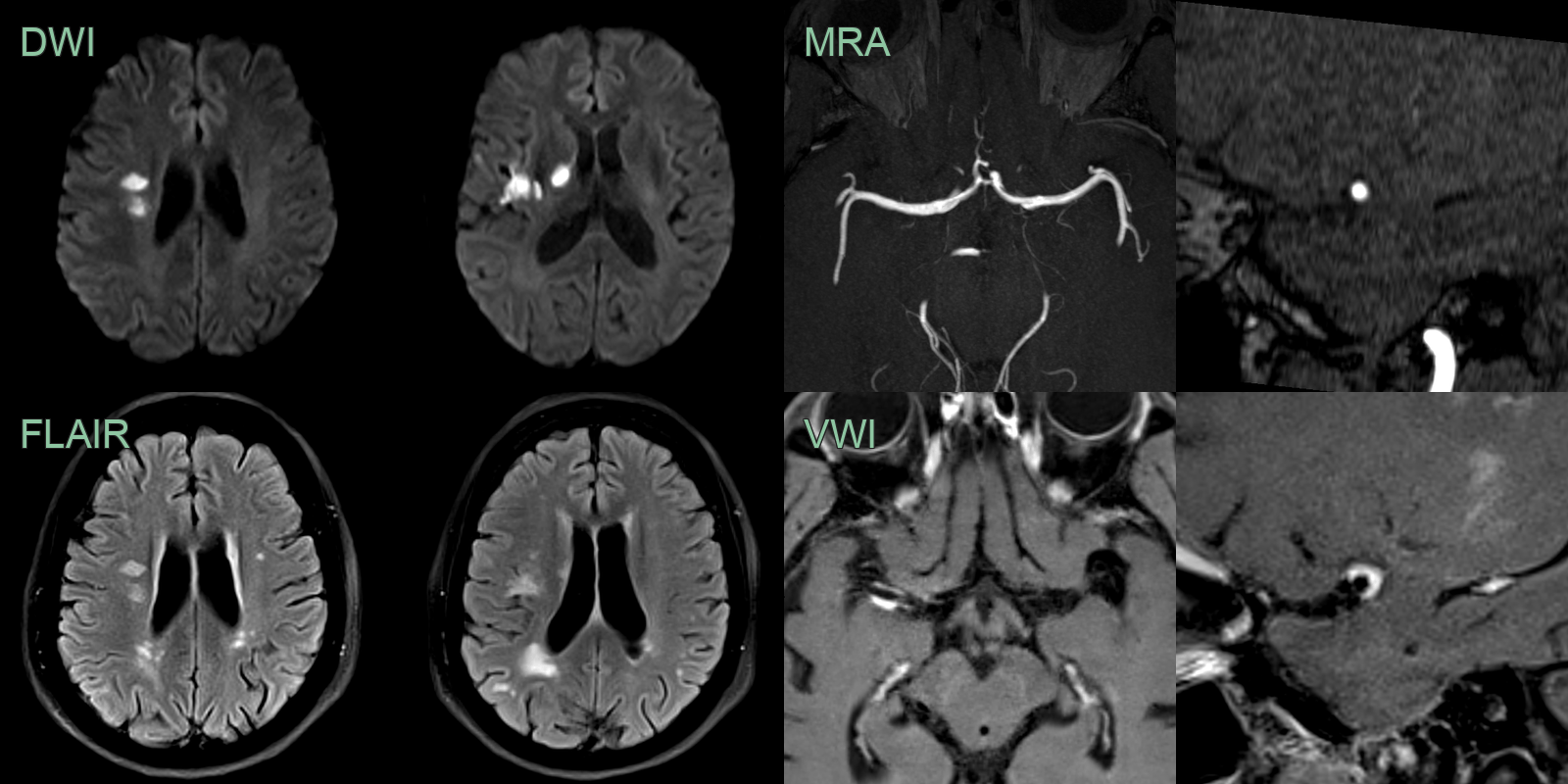
- 50-year-old patient presented with visual disturbance and left sided weakness.
- CSF PCR was positive for VZV.
- MRI showed multiple left MCA territory infarcts.
- There wasthick eccentric enhancement on the right MCA but no stenosis initially.
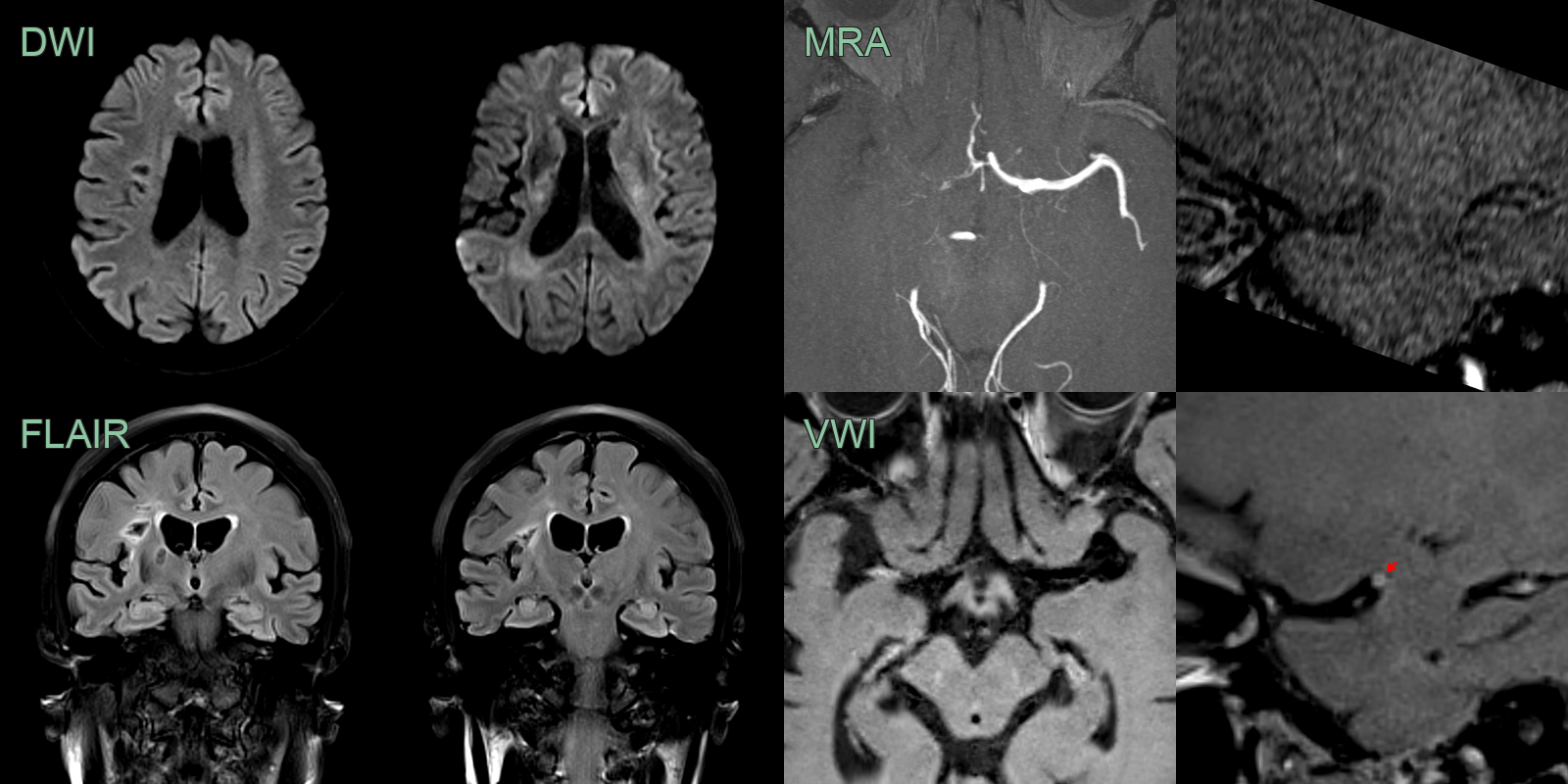
- After 5 months and following steroid therapy, the enhancement associated with the vasculopathy regressed but a severe long segment stenosis developed. This only slightly improved (trace of flow related signal) on further follow-up MRA (not shown).
Treatment¶
- Antiviral therapy:
- Intravenous aciclovir (10-15 mg/kg every 8 hours) for 14 days
- Consider oral valaciclovir for maintenance therapy
- Adjunctive corticosteroids:
- Controversial, but may help reduce inflammation
- Prednisone 1 mg/kg/day, tapered over 4-6 weeks
- Antiplatelet therapy:
- Aspirin or clopidogrel to prevent thrombotic complications
- Management of complications:
- Stroke care protocols as appropriate
- Rehabilitation for neurological deficits
- Long-term follow-up:
- Serial neuroimaging to monitor disease progression
- Neurological assessments to evaluate recovery
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Primary Angiitis of CNS (PACNS) | Multifocal arterial beading on angiography involving small and medium vessels; vessel wall enhancement on high-resolution MRI; no supraclinoid ICA predilection |
| Atherosclerosis | Calcified eccentric plaques on CTA; large vessel involvement with stenosis; no vessel wall inflammation on MRI |
| Reversible Cerebral Vasoconstriction Syndrome | Multifocal segmental arterial narrowing reversible on follow-up MRA within 12 weeks; no vessel wall enhancement |
| Moyamoya Disease | Bilateral ICA terminus occlusion with "puff of smoke" lenticulostriate collaterals on DSA; no unilateral large vessel predilection |
| Neurosyphilis | Vessel wall thickening and enhancement on high-resolution MRI; may appear identical to VZV vasculitis; meningeal enhancement |
| Cerebral Venous Thrombosis | Filling defects in dural venous sinuses on CT/MR venography; venous rather than arterial territory infarcts |