Warthin's tumour¶
Summary
- Benign neoplasm of the salivary glands, predominantly affecting the parotid gland
- Characterised by oncocytic epithelial cells and lymphoid stroma
- Typically presents as a slow-growing, painless mass in older male patients
Pathophysiology¶
- Derived from heterotopic salivary gland tissue within lymph nodes
- Composed of:
- Bilayered oncocytic epithelium forming cystic spaces
- Lymphoid stroma with germinal centers
- Etiology remains unclear, but smoking is a significant risk factor
Demographics¶
- Most common in the 6th-7th decades of life
- Male predominance (4:1 male to female ratio)
- Higher incidence in smokers
- Accounts for 5-10% of all parotid gland tumours
Diagnosis¶
- Clinical presentation:
- Painless, slow-growing mass in the parotid region
- Occasionally bilateral (5-14% of cases)
- Fine-needle aspiration cytology (FNAC):
- Oncocytic cells and lymphocytes in a proteinaceous background
- Diagnostic accuracy of 90%
Imaging¶
- Ultrasound:
- Well-defined, hypoechoic mass with internal echogenic areas
- Increased vascularity on colour Doppler
- CT:
- Well-circumscribed, homogeneous mass
- Enhancement less than normal parotid tissue
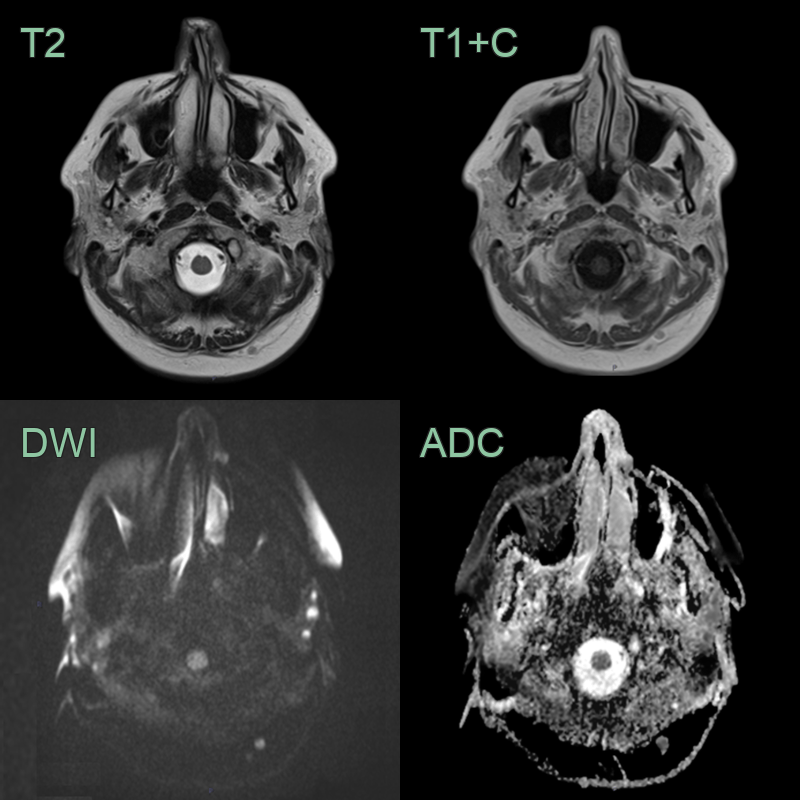
- MRI:
- T1: Low to intermediate signal intensity
- T2: Heterogeneous high signal intensity
- "Cluster of grapes" appearance on T2-weighted images
- Nuclear Medicine:
- Increased uptake on Technetium-99m pertechnetate scintigraphy
Treatment¶
- Surgical excision:
- Superficial parotidectomy is the standard treatment
- Enucleation may be considered for small, superficial tumours
- Observation:
- May be appropriate in elderly patients or those with significant comorbidities
- Prognosis:
- Excellent, with low recurrence rates (<2%)
- Malignant transformation is extremely rare (<1%)
- Follow-up:
- Regular clinical examinations and imaging studies to monitor for recurrence
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Pleomorphic adenoma | Lacks lymphoid stroma; appears more heterogeneous on imaging |
| Basal cell adenoma | No cystic components; solid appearance on imaging |
| Oncocytoma | Lacks lymphoid stroma; appears as a solid mass without cystic spaces |
| Mucoepidermoid carcinoma | More infiltrative growth; may show enhancement on contrast imaging |
| Lymphoma | Typically involves multiple lymph nodes; homogeneous appearance |
| Branchial cleft cyst | Unilocular cyst; lacks solid components |
| Lipoma | Fat signal on MRI; homogeneous appearance |
| Schwannoma | Eccentric growth pattern; may show cystic degeneration but lacks oncocytic epithelium |
| Metastatic lymph node | Irregular margins; central necrosis; no mixed cystic-solid morphology of parotid origin |
| Chronic sialadenitis | Diffuse gland involvement; no discrete mass |