X-Linked Adrenoleukodystrophy¶
Summary
- X-linked peroxisomal disorder causing accumulation of very long-chain fatty acids (VLCFAs) in tissues, leading to progressive demyelination of cerebral white matter and adrenal insufficiency
- Presents in childhood with behavioural changes, cognitive decline, and visual/auditory deficits, progressing to severe neurologic disability
- MRI shows characteristic posterior-predominant white matter demyelination with enhancement at the advancing edge
Pathophysiology¶
- Mutation in ABCD1 gene on chromosome Xq28 encoding adrenoleukodystrophy protein (ALDP)
- Defective peroxisomal beta-oxidation leads to accumulation of VLCFAs (C24:0 and C26:0)
- Three main phenotypes:
- Childhood cerebral form (35-40%)
- Adrenomyeloneuropathy (40-45%) - adult onset with spinal cord involvement
- Addison disease only (10%)
- Inflammatory demyelination with perivascular lymphocytic infiltration
- Progressive destruction of myelin with relative sparing of U-fibres initially
- Zones of demyelination:
- Central zone: gliosis and cavitation
- Intermediate zone: active inflammation and demyelination
- Peripheral zone: active demyelination with gadolinium enhancement
Demographics¶
- X-linked recessive inheritance pattern
- Incidence: 1 in 17,000 males
- Childhood cerebral form: onset 4-10 years (peak 7 years)
- Adrenomyeloneuropathy: onset 20-30 years
- Female carriers: usually asymptomatic or mild symptoms after 40 years
- No ethnic predilection
Diagnosis¶
- Clinical presentation:
- Behavioural changes, ADHD-like symptoms
- Progressive cognitive decline
- Visual and auditory deficits
- Gait disturbances
- Seizures in advanced stages
- Adrenal insufficiency (may precede neurologic symptoms)
- Laboratory findings:
- Elevated plasma VLCFAs (C26:0, C24:0/C22:0 ratio)
- ACTH stimulation test abnormal in 85%
- Genetic testing for ABCD1 mutations
- Loes score: MRI-based severity scoring system (0-34 points)
Imaging¶
- MRI findings:
- T2/FLAIR: symmetric hyperintense signal in parieto-occipital white matter
- Splenium of corpus callosum involved early
- Progression in centrifugal pattern
- Corticospinal tract involvement (pyramidal tract sign)
- Auditory pathway involvement (lateral lemniscus, inferior colliculus)
- T1: hypointense in areas of demyelination
- T1+C: peripheral enhancement at advancing edge ("leading edge enhancement")
- Indicates active inflammation
- Correlates with disease progression
- DWI: restricted diffusion at actively demyelinating edge
- Facilitated diffusion in central necrotic zones
- SWI: usually normal, occasional microhaemorrhages in severe cases
- MR Spectroscopy: elevated choline, decreased NAA, presence of lipid/lactate peaks
- Pattern variations:
- 80% posterior predominant (parieto-occipital)
- 20% frontal predominant
- Rare: unilateral, cerebellar, or isolated corticospinal tract involvement
- CT findings:
- Symmetric hypodensity in periventricular white matter
- Calcifications rare
- Less sensitive than MRI for early detection
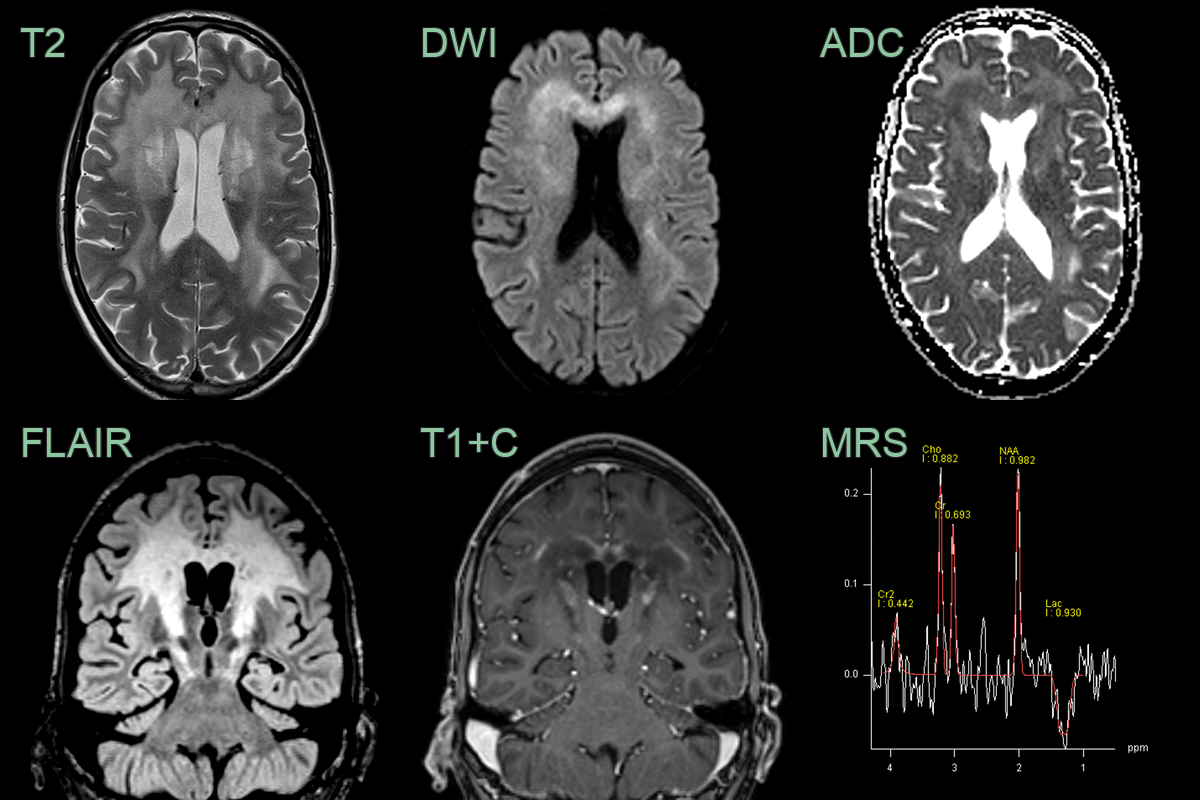
- A 35-year-old male presented with cognitive impairment and personality change.
- Imaging showed a diffuse anterior-predominant leukoencephalopathy with a centrifugal pattern of enhancement.
- MR spectroscopy showed a reduction in NAA and the presence of lactate.
- X-ALD was confirmed on identification of a hemizygous ABCD1 pathogenic variant on molecular genetic testing.
Treatment¶
- Hematopoietic stem cell transplantation (HSCT):
- Most effective if performed early (Loes score <9)
- Can halt progression in 80-90% if done in early stages
- High morbidity/mortality if performed in advanced disease
- Lorenzo's oil:
- Combination of oleic and erucic acids
- May lower VLCFA levels but limited clinical efficacy
- Potential benefit in asymptomatic patients
- Gene therapy:
- Lent
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Adrenomyeloneuropathy | Predominantly spinal cord dorsal column involvement with minimal cerebral white matter changes; no posterior parieto-occipital predominance or garland enhancement |
| Multiple sclerosis | Periventricular and juxtacortical lesions without posterior predominance; calloso-septal interface lesions; short cord lesions; no zonal garland enhancement |
| Metachromatic leukodystrophy | Frontal and parietal predominance with "tigroid" or "leopard skin" T2 pattern; corticospinal tract involvement; no garland enhancement zone |
| Krabbe disease | Peritrigonal white matter T2 signal with corticospinal tract and cerebellar involvement; thalamic T2 hypointensity; optic radiation changes |
| Alexander disease | Frontal predominance with basal ganglia and thalamic involvement; periventricular garland enhancement can overlap but anterior distribution |
| Acute disseminated encephalomyelitis (ADEM) | Bilateral multifocal white matter lesions involving grey and white matter; incomplete ring enhancement; no posterior predominant zonal pattern |
| Pelizaeus-Merzbacher disease | Hypomyelination pattern with reduced white matter T2 signal rather than T2 hyperintensity; tigroid pattern; no enhancement |