Choroid fissure cyst¶
Summary
- Benign, cerebrospinal fluid–containing neuroepithelial cyst arising within the choroidal fissure of the medial temporal lobe
- Almost always an incidental, asymptomatic finding that follows CSF signal on all sequences
- No treatment or follow-up is required when the imaging features are typical
Pathophysiology¶
- Arises within the choroidal fissure, a CSF-containing cleft in the medial temporal lobe between the fornix and the thalamus/temporal horn, along the course of the choroid plexus
- Considered a neuroepithelial (ependymal-lined) cyst formed during infolding of the choroid plexus in embryological development
- Contains clear CSF-like fluid and does not communicate abnormally with the ventricular system
- Non-neoplastic and does not typically enlarge over time
Demographics¶
- Common incidental finding seen across all age groups
- No significant sex predilection
- Increasingly detected owing to the widespread use of high-resolution MRI
Diagnosis¶
- Almost always discovered incidentally on imaging performed for unrelated reasons
- Rarely symptomatic; large cysts have occasionally been associated with:
- Headache
- Seizures, when located in the mesial temporal lobe
- Diagnosis is made on the characteristic imaging appearances; histology is seldom required
Imaging¶
- Location: medial temporal lobe, within the choroidal fissure, typically ovoid or spindle-shaped and oriented along the fissure
- CT:
- Well-defined, rounded CSF-density lesion
- No calcification and no surrounding oedema
- MRI:
- Follows CSF signal on all sequences (T1 hypointense, T2 hyperintense)
- Suppresses completely on FLAIR
- No restricted diffusion
- No enhancement following contrast
- No mass effect, with normal adjacent brain parenchyma
- Differential diagnosis:
- Epidermoid cyst
- Arachnoid cyst
- Dilated perivascular spaces
- Cystic neoplasm
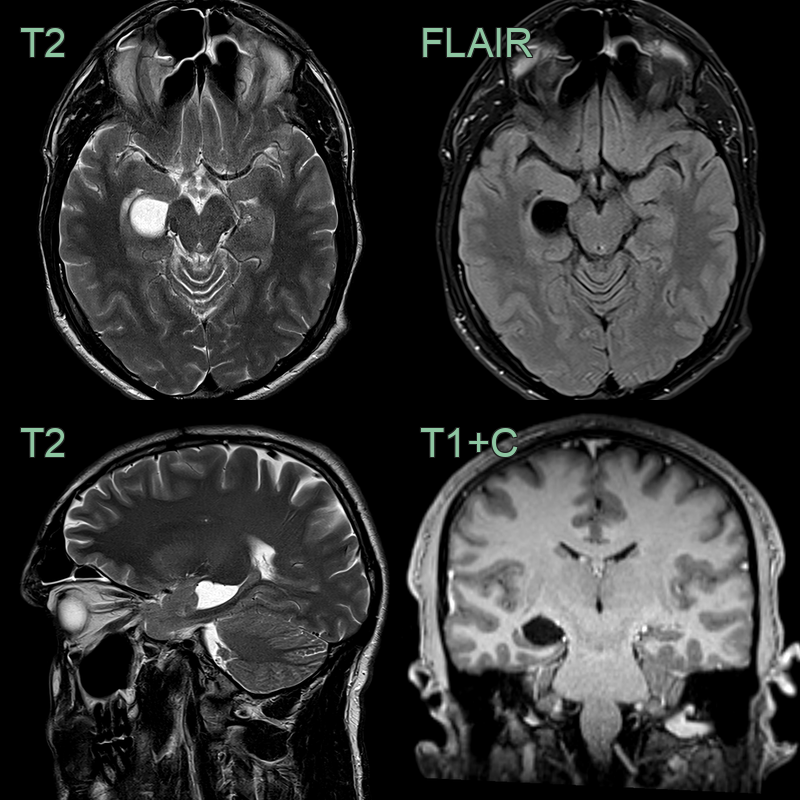
- A 40-year-old patient presenting with a headache had an incidental non-enhancing cyst expanding the choroidal fissure. The lesion followed CSF signal on all sequences and suppressed completely on FLAIR.
Treatment¶
- No treatment is required for typical, asymptomatic cysts
- No imaging follow-up is necessary once the diagnosis is confident
- Surgical fenestration is reserved for the rare symptomatic or enlarging lesion
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Epidermoid cyst | Does not suppress on FLAIR; characteristically restricts on diffusion-weighted imaging |
| Arachnoid cyst | Similar CSF signal but sited in typical arachnoid spaces (e.g., middle cranial fossa) rather than the choroidal fissure |
| Dilated perivascular spaces | Cluster along penetrating vessels (e.g., basal ganglia, midbrain); typically smaller and multiple |
| Neuroglial (glioependymal) cyst | Indistinguishable by signal; located within parenchyma rather than the choroidal fissure |
| Cystic neoplasm (e.g., DNET, low-grade glioma) | Solid or enhancing components; does not follow CSF signal; may exert mass effect |
| Neurocysticercosis (vesicular stage) | Scolex within the cyst; may enhance; often multiple |
| Hippocampal sulcus remnant cysts | Row of tiny cysts along the hippocampal sulcus; smaller |